Case #1350 · Montreal
Direct-to-Implant Reconstruction

Drag the handle to compare. Click anywhere to jump.
Additional views




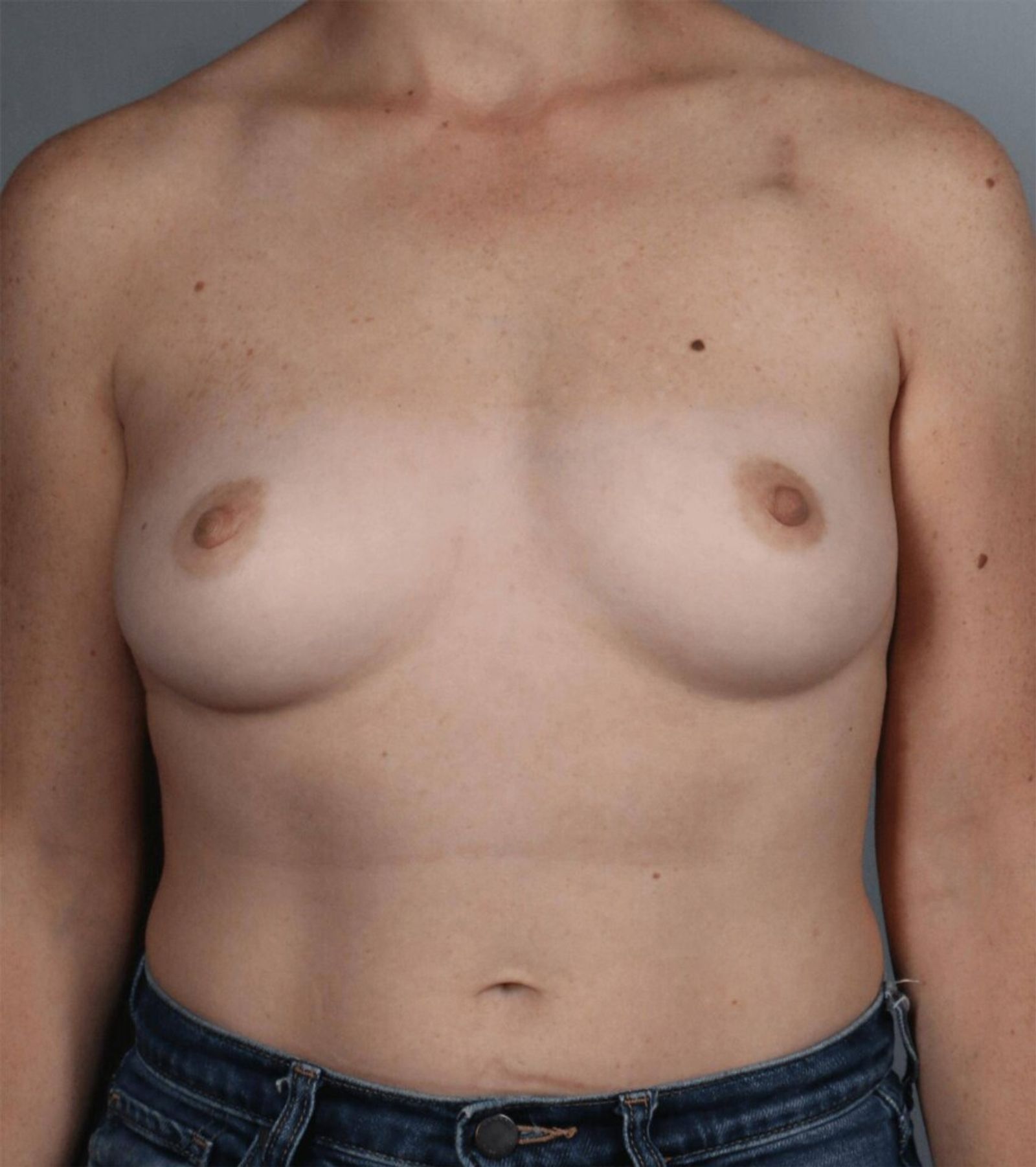
This 35-year-old patient from Montreal was diagnosed with cancer in the right breast. After undergoing a bilateral mastectomy, Dr. Cassileth performed direct-to-implant breast reconstruction. She placed 405cc silicone implants and used dermal matrix for added support.
Continued care
Recommended aftercare, skincare, and MedSpa services for Direct-to-Implant Reconstruction.
- Lymphatic drainage massage starting week 2
- Compression garment for 4–6 weeks
- Scar management protocol at 3 weeks
- Hyperbaric oxygen therapy to raise tissue oxygen and support skin and incision healing, particularly with prior radiation or a compromised blood supply
- SkinCeuticals C E Ferulic for scar healing
- Medical-grade silicone sheeting
- SPF 50+ on incision sites
- Laser or microneedling for scar refinement after 3 months
- LED light therapy to accelerate healing
- Indiba radiofrequency for tissue recovery
- Coordination
Imaging cadence reviewed against the oncology plan at the 3-month visit.
Post-mastectomy patients stay on a long-term surveillance pathway.
- Aftercare
Early lymphatic massage protocol initiated in the first week of recovery.
Lymphatic disruption from axillary work makes early drainage more valuable.
- Skincare
SPF 50+ on incisions daily for the first year; younger skin pigments scars more reliably under UV.
Younger skin pigments scars more reliably under sun exposure.
Why this approach
The decisions that shaped this surgical plan.
- Approach driven by the oncologic priority first: incisions and tissue handling chosen to give the oncology team the access they need, then to set up the cleanest reconstructive canvas.
- Surgical plan calibrated against the opposite side. Final shape, scar position, and volume targeted to match, not to a generic ideal.
Pre-op preparation
What to do before surgery. Specific to this case.
- Stop NSAIDs, aspirin, and high-dose fish oil two weeks before surgery; the surgical team provides a full medication list at the pre-op visit.
- Full nicotine cessation 6 weeks pre- and post-op. This includes vapes and nicotine replacement products; the constriction effect is the same.
- No overhead clothing for 3 weeks. Stock front-zip tops, supportive sports bras (post-clearance), and the drain pouches we provide.
- Day-of transport and an overnight companion (24 hours minimum) are required for discharge.
- Surgical date confirmed against oncology pathway. Imaging and pathology results are reconciled by the team at the pre-op visit.
Recovery timeline
Milestones specific to this case. Individual recovery varies.
- Day 1–7
Drains in place, restricted lifting (nothing over 5 lb), and rest. Pain management is shifted off narcotics within the first 72 hours when possible.
- Week 2
Patients off prescription pain medication, walking 1–2 miles daily, and back to most light household activity.
- Week 4
Light cardio and most desk-work activities cleared. Lifting limit increases to 15 lb. Scar massage typically starts now.
- Week 6
Most physical restrictions lift. Return to strength training, full-impact cardio, and overhead lifting.
- Month 3
First major reconstruction assessment. Tissue softens, surveillance imaging if indicated coordinates here.
- Month 6
Final aesthetic emerges. Last-mile adjustments (fat grafting, nipple reconstruction) typically scheduled now.
“Reconstructing the breasts at the same time as mastectomy eliminates the risks of multiple surgeries and, more importantly, helps minimize the sense of loss.”
Dr. Lisa Cassileth





